
Disclaimer: This guide provides recruitment strategies based on 2026 market data and state-specific incentive programs. Always verify current grant availability with state health departments and the Health Resources and Services Administration (HRSA).
This guide provides rural clinic owners and HR leaders with a data-backed roadmap to bridge the 2026 provider gap. Y
ou will learn how to leverage Hub-and-Spoke telehealth models, access state-specific financial incentives, and use Lifestyle Arbitrage to win talent from metropolitan competitors.
At-a-Glance: The Rural Recruitment Cheat Sheet
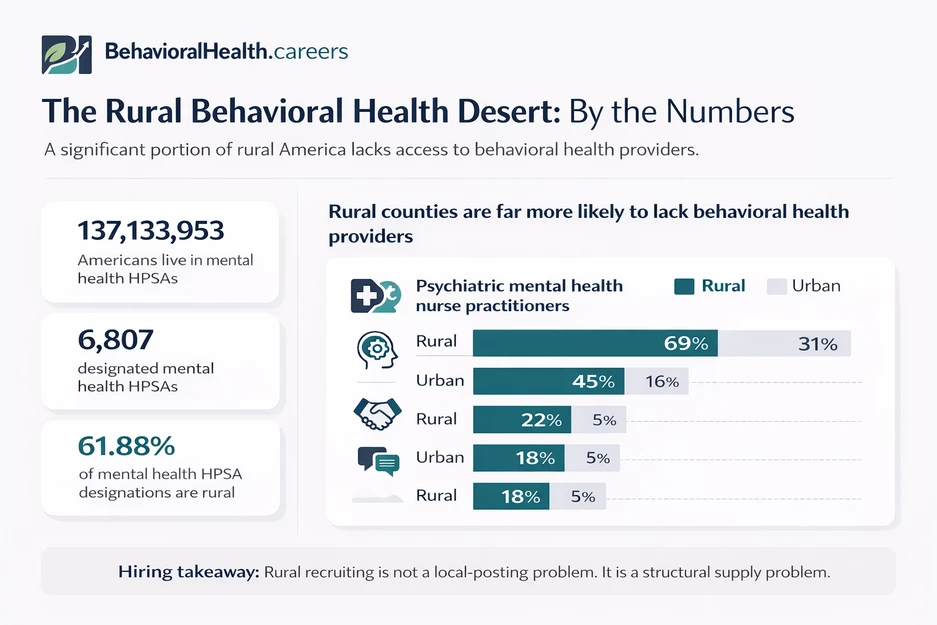
- The Problem: 130 million Americans live in "Behavioral Health Deserts" where provider density is up to 65% lower than urban centers.
- The 2030 Outlook: Telehealth will shift from an "alternative" to the primary delivery method for rural care within five to ten years.
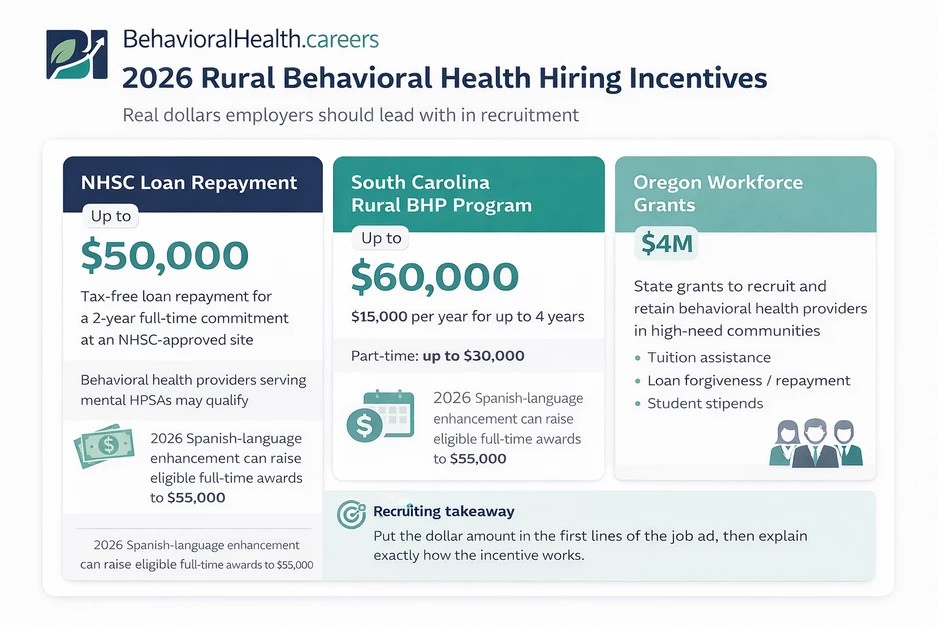
- The Financial Edge: Incentives in states like South Carolina ($60,000) and Oregon ($4M grant pool) are currently active for rural practitioners.
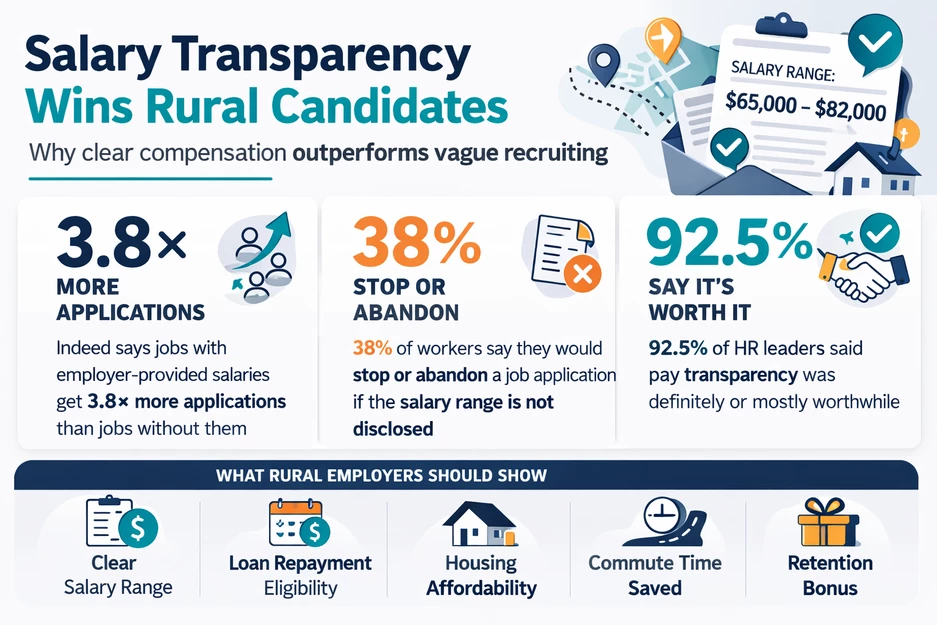
- The Secret Weapon: Use Salary Transparency to highlight "purchasing power" rather than just the gross number.
Understanding the Behavioral Health Desert
The "Behavioral Health Desert" is not a metaphor: it is a measurable workforce crisis. As we detailed in our Workforce Outlook, the geographic maldistribution of providers is the single largest barrier to care in 2026.
Data shows that while social workers have the most balanced rural coverage, psychiatric nurse practitioners and psychologists are nearly non-existent in over 45% of rural counties [[1]].
For a rural employer, this means you are not just competing with the clinic down the road; you are competing with every urban health system offering remote flexibility.
What this means for you: Traditional "post and pray" recruiting is dead in rural markets. You must pivot from finding local talent to importing it: either physically or virtually.
The Telehealth Pivot: Embracing the Hub-and-Spoke Model
The next five to ten years will see a total reorganization of rural care delivery. Instead of trying to staff a remote clinic with a full suite of onsite specialists, successful employers are adopting the Hub-and-Spoke model.
The Setup:
- The Hub: A centralized location (often in a mid-sized city) where specialized clinicians (LCSWs, Psych NPs, BCBAs) operate.
- The Spoke: Your rural clinic, staffed by Direct Support Professionals (DSPs), Registered Behavior Technicians (RBTs), or Medical Assistants who facilitate the "human" side of the visit.
This model solves the "isolation" problem that drives clinician turnover. By allowing specialists to live in areas with more amenities while treating rural patients via high-definition tele-suites, you eliminate the relocation barrier entirely.
Hiring implications: Start recruiting for "Telehealth-Hybrid" roles. You need local "Spoke" staff who are tech-savvy and urban "Hub" staff who are culturally competent in rural nuances.
Leveraging 2026 Financial Incentives
If you are not mentioning state and federal money in your job titles, you are losing candidates. 2026 has seen a massive influx of "carrots" for rural providers.
National Health Service Corps (NHSC):
Ensure your facility is NHSC-approved. This allows your hires to access up to $50,000 in tax-free loan repayment for a two-year commitment.
For a clinician with six-figure student debt, this is more valuable than a signing bonus. Check eligibility at https://behavioralhealth.careers/blog/student-loan-repayment-for-behavioral-health-professionals.
State-Specific Powerhouse Programs:
- South Carolina: The Rural BHP program offers up to $60,000 for behavioral health providers committing to underserved areas.
- Oregon: The state recently allocated a $4M rural workforce grant specifically for retention and recruitment in non-metro regions.
- Colorado: Facing a projected deficit of 4,400 workers, the state is offering aggressive reimbursement bumps for rural Medicaid providers [[5]].
Action Step: Include the specific dollar amount of these grants in the first two sentences of your job description. Example: "Join our team and qualify for $60k in SC Rural BHP incentives."
The 'Lifestyle Arbitrage' Play: Using Salary Transparency
Rural employers often feel they cannot compete with $120k urban salaries. This is a misconception.
Using Salary Transparency is your greatest tool for demonstrating Lifestyle Arbitrage.
The Math of Transparency:
An $85,000 salary in a rural county often carries the same "standard of living" as $160,000 in San Francisco or NYC. When you list a salary range on BehavioralHealth.careers, you aren't just showing a number; you are showing the ability to own a home, avoid a commute, and build actual wealth.
What to include in your pitch:
- Median Home Price: Contrast your local average with the national average.
- Commute Time: Calculate the "reclaimed life hours" (e.g., "Save 10 hours a week on I-95").
- No State Income Tax: If applicable (e.g., Texas, Florida, Tennessee), emphasize this as a 10% effective raise.
Special Considerations for Rural ABA and Autism Services
Recruiting for Applied Behavior Analysis (ABA) in rural areas is uniquely difficult because of the travel requirements for RBTs and the supervision requirements for BCBAs.
Address the Travel Burnout:
Rural RBTs often spend more time in their cars than in sessions. If you want to retain them, you must pay for travel time at the full hourly rate: not a "travel rate."
- Action: Provide a company vehicle or a significant monthly gas stipend.
- Action: Use "Cluster Scheduling" to ensure RBTs see multiple clients in the same geographic "zone" on the same day.
Virtual Supervision Models:
BCBAs are the rarest commodity in rural health autism and ABA settings.
Use Virtual Supervision to allow a BCBA in a different city to supervise rural RBTs. Ensure your "Spoke" clinics have dedicated tablets and HIPAA-secure software to make this seamless.
Search our current listings for examples of how to structure these roles:
Actionable Guidance: Relocation vs. Retention
Should you spend $10,000 to move someone to town, or $10,000 to keep them there? Data suggests a shift toward Retention Stipends.
The Relocation Trap:
Paying for a move is a "one-and-done" incentive. If the clinician doesn't like the town, they leave as soon as the contract is up.
The Retention Stipend Strategy:
Instead of a lump-sum relocation bonus, offer a "Rural Longevity Bonus."
- Year 1: $5,000 bonus.
- Year 2: $7,500 bonus.
- Year 3: $10,000 bonus + 1 month paid sabbatical.
This structure rewards the behavior you actually want: community integration.
Employer Checklist: Rural Recruitment Audit
[ ] Update Job Titles: Add "Loan Repayment Eligible" or "Remote Hybrid" to every title.
[ ] Audit Your Salary: Is your range clearly visible? Transparency increases applicant flow by up to 30%.
[ ] Map the Incentives: Create a 1-page PDF for candidates explaining the NHSC and state grants.
[ ] Test Your Tech: Can a clinician perform 100% of their documentation and 50% of their sessions remotely?
[ ] Local Partnership: Do you have a "Community Welcome" package (local gym membership, intro to the school board, etc.)?
The Reality Check
Rural recruitment is a marathon, not a sprint. You are fighting a national shortage that will persist through 2030.
However, by leveraging Hub-and-Spoke models and being radically transparent about purchasing power, you can attract clinicians who are tired of the urban grind.
Ready to find your next rural provider? Post your first job for free on our specialized board and tap into a network of clinicians looking for their next move.