Primary care clinics are drowning in mental health demand they weren't built to handle. Emergency departments are boarding psychiatric patients for days. Therapists have three-month wait lists. The traditional "refer out" model is broken.
The Collaborative Care Model (CoCM) fixes this by embedding mental health care directly into primary care settings. The Collaborative Care Model improves patient outcomes and increases satisfaction for both patients and providers.
And it's not a referral system. It's a team-based integration model with an evidence base stronger than almost any other intervention in behavioral health: 80+ randomized controlled trials proving it works across depression, anxiety, PTSD, and substance use disorders.
For healthcare systems, the ROI is measurable: $6.50 return for every $1 spent.
For employers hiring in this space, CoCM creates entirely new job categories with sustainable caseloads and billable structures.
If you're a clinic administrator, a psychiatric consultant, or a care manager trying to understand where the industry is headed in 2026, this is the model driving hiring and reimbursement.
At a Glance: What You Need to Know About CoCM
The Structure: A three-person care team (Primary Care Provider, Behavioral Health Care Manager, Psychiatric Consultant) treats mental health conditions in the same clinic where patients get their annual physicals.
The ROI: Medicare and most commercial payers now reimburse CoCM through specific billing codes. Clinics see cost savings within 6 months and sustained reductions in total healthcare spending for up to 4 years.
The Hiring Impact: CoCM creates demand for Behavioral Health Case Managers (a role that didn't exist at scale five years ago) and remote Psychiatric Consultants (which solves the psychiatrist shortage without requiring patients to travel).
Who This Guide Is For:
- Health system administrators evaluating integrated care models
- Psychiatrists and psychiatric nurse practitioners exploring consulting roles
- Licensed therapists, social workers, and counselors considering care management positions
- Employers hiring for CoCM teams and unsure what credentials to require
How CoCM Actually Works: The Three-Role Framework
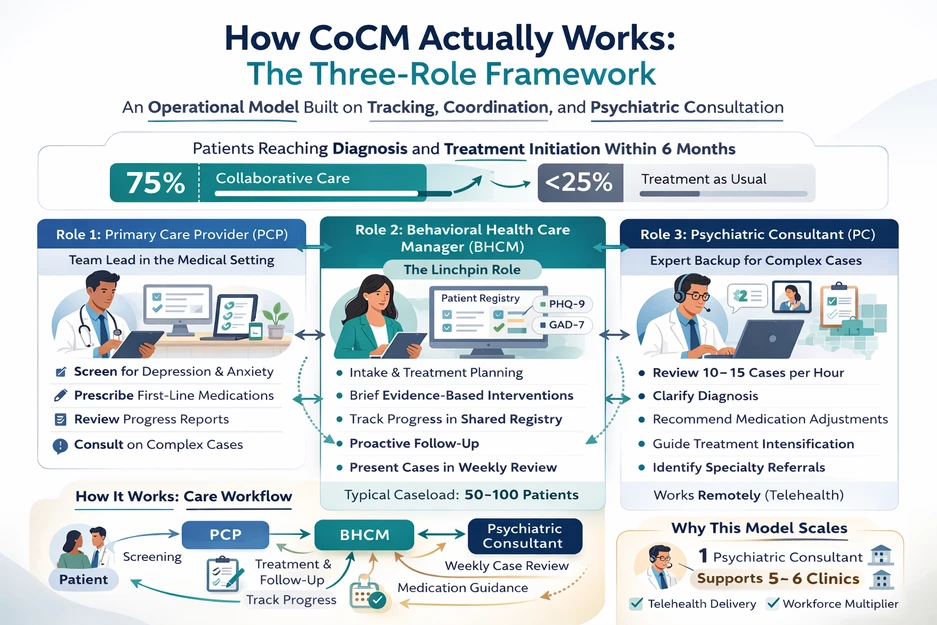
CoCM is not a therapy program. It's an operational care model built on systematic tracking and interdisciplinary consultation.
Patients treated with Collaborative Care reach a diagnosis and initiate treatment within 6 months 75% of the time, compared to less than 25% of patients receiving treatment as usual.
Role 1: Primary Care Provider (PCP)
The PCP, usually a physician, nurse practitioner, or physician assistant, leads the team and prescribes psychiatric medications when appropriate. They don't need specialty mental health training.
The model works because the PCP delegates care coordination and gets expert backup from the psychiatric consultant.
What they do:
- Conduct initial depression or anxiety screenings during routine visits
- Prescribe first-line psychiatric medications (SSRIs, SNRIs, buspirone)
- Review patient progress reports and patient outcomes from the care manager
- Consult with the psychiatric consultant on complex cases
Role 2: Behavioral Health Care Manager (BHCM)
This is the linchpin role. The BHCM is typically a licensed clinical social worker (LCSW), licensed professional counselor (LPC), or registered nurse (RN) with behavioral health training.
They manage a caseload of 50–100 patients, tracking symptoms using standardized scales (PHQ-9 for depression, GAD-7 for anxiety) and delivering brief evidence-based interventions.
Meta-analyses indicate CoCM is more effective than standard care for treating depression and anxiety.
What they do:
- Conduct intake assessments and build treatment plans
- Deliver behavioral activation, motivational interviewing, or brief cognitive-behavioral therapy
- Track patient progress in a shared registry
- Follow up proactively with patients who miss appointments or aren't improving
- Present cases to the psychiatric consultant during weekly caseload reviews
Hiring Note: Most CoCM programs require the BHCM to hold an independent clinical license, though some use master's-level clinicians under supervision. If you're recruiting for this role, look for candidates with experience in brief interventions and comfort working in fast-paced medical settings.
Role 3: Psychiatric Consultant (PC)
The psychiatric consultant, almost always a psychiatrist or psychiatric-mental health nurse practitioner (PMHNP), does not see patients directly in what is often a form of primary care behavioral health.
Instead, they review cases with the care manager, recommend medication adjustments, and guide treatment intensification.
What they do:
- Review 10–15 cases per hour during structured caseload consultation sessions
- Provide diagnostic clarification and medication recommendations to the PCP
- Identify patients who need specialty referrals (e.g., intensive outpatient programs)
- Work remotely via telehealth in most implementations
Why This Model Works for Recruitment: One psychiatric consultant can support 5–6 primary care clinics through telehealth. In states like South Carolina, where 14 of 46 counties have zero psychiatrists, this multiplier effect makes psychiatric expertise accessible without requiring relocation.
The 2026 Business Case: Billing Codes and Financial Sustainability
CoCM was a research model until 2017, when CMS created reimbursement codes that made it financially viable at scale.
As of 2026, most commercial payers and 40+ state Medicaid programs cover CoCM services for both general and specialty mental health care.
The Billing Codes You Need to Know
- CPT 99492 , Psychiatric Collaborative Care Management, first 70 minutes
This code covers the initial month of care coordination: intake, treatment planning, and the first psychiatric consultation. Reimbursement typically ranges from $130–$160 depending on payer.
- CPT 99493 , Subsequent months, minimum 60 minutes
Used for ongoing care management after the first month. Pays approximately $110–$140.
- CPT 99494 , Additional 30 minutes beyond 60-minute threshold
An add-on code for complex patients requiring extra care manager time. Pays approximately $55–$70.
- G2214 , Behavioral Health Integration, 20 minutes
A new 2026 code for brief check-ins and care coordination that don't meet the full CoCM threshold. Used for transitional care or patients in maintenance phases.
Advanced Primary Care Management or APCM
CMS introduced APCM codes in 2025 to support practices that integrate behavioral health alongside chronic disease management.
These codes bundle mental health care coordination with diabetes, hypertension, and cardiovascular management.
If your clinic is already managing complex medical patients, APCM allows you to bill for integrated behavioral health without separate documentation workflows.
What This Means for Hiring: Clinics implementing CoCM or APCM need care managers who can document time spent per patient, use standardized outcome measures, and present cases during psychiatric consultation sessions. When you're posting jobs, specify that candidates should have experience with registry-based care and measurement-based treatment.
How CoCM Solves the 2026 Recruitment Crisis
The behavioral health workforce shortage is, in part, about volume. It is also about distribution and sustainability.
The Psychiatrist Multiplication Effect
There are approximately 28,000 psychiatrists in the US serving a population that needs far more psychiatric care than 28,000 providers can deliver one-on-one.
CoCM turns one psychiatrist into a force multiplier: instead of seeing 15 patients per day in 50-minute sessions, a psychiatric consultant can support 500–600 patients by advising care teams.
Recruitment Implication: If you're hiring a psychiatric consultant for a CoCM program, emphasize the caseload leverage and the ability to practice at the top of license without the administrative burden of direct patient scheduling for a wide array of behavioral health conditions. Many psychiatrists burned out on traditional clinic models find CoCM consulting sustainable and intellectually engaging.
The Care Manager Career Path
Five years ago, "Behavioral Health Care Manager" wasn't a distinct job title. Now it's one of the fastest-growing roles in integrated care.
LCSWs and LPCs who spent years in private practice managing 25 to 30 clients per week can transition to CoCM roles with structured caseloads, predictable schedules, and built-in psychiatric backup.
What to Highlight in Job Posts:
- Defined caseloads: Care managers typically handle 50–100 active patients, not the 30+ weekly therapy sessions of traditional outpatient roles
- Team-based support: Weekly psychiatric consultation eliminates the isolation of solo practice
- Measurement-based care: Progress is tracked using validated tools, which appeals to clinicians who value outcome data
- No on-call or crisis work: CoCM operates during clinic hours, with PCP coverage for urgent needs
Rural Access and Telehealth Expansion
CoCM is the most effective model for expanding psychiatric access in underserved areas.
Federally Qualified Health Centers (FQHCs) in rural Texas, South Carolina, and Montana have used telehealth-enabled CoCM to bring psychiatric consultation to counties that haven't had a resident psychiatrist in over a decade.
If you're recruiting for rural or semi-rural clinics, remote psychiatric consultant roles are your highest-leverage hire. One consultant working from anywhere can support clinics across multiple states (subject to licensure compacts like PSYPACT).
Implementation Checklist: What You Need Before You Hire
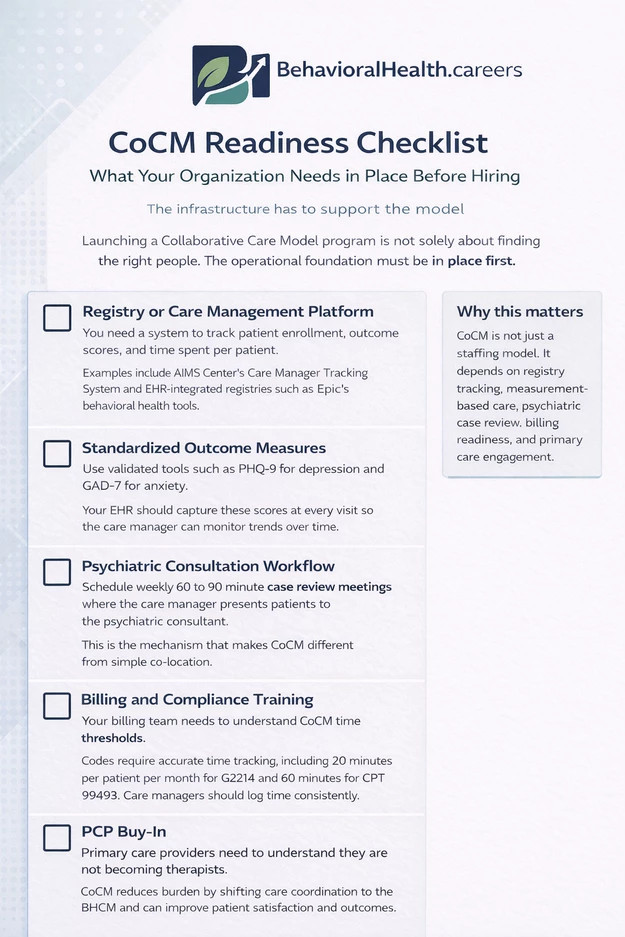
Launching a CoCM program is not solely about finding the right people. The infrastructure has to support the model.
[ ] Registry or Care Management Platform
You need a system to track patient enrollment, outcome scores, and time spent per patient. Popular platforms include AIMS Center's Care Manager Tracking System and EHR-integrated registries like Epic's Behavioral Health module.
[ ] Standardized Outcome Measures
CoCM requires validated tools: PHQ-9 for depression, GAD-7 for anxiety. Your EHR needs to capture these scores at every visit so the care manager can monitor trends.
[ ] Psychiatric Consultation Workflow
Schedule weekly 60–90 minute case review meetings where the care manager presents patients to the psychiatric consultant. This is not optional. It's the mechanism that makes CoCM different from co-location.
[ ] Billing and Compliance Training
Your billing team needs to understand CoCM time thresholds. Codes require a minimum of 20 minutes per patient per month for G2214 and 60 minutes for CPT 99493. Train care managers to log their time accurately.
[ ] PCP Buy-In
Primary care providers need to understand they're not becoming therapists. CoCM reduces their burden by offloading care coordination to the BHCM. If your PCPs are skeptical, show them the data: practices report improved patient satisfaction and reduced no-show rates after implementing CoCM.
Common Questions and Myths About CoCM
"Isn't this just co-location with a fancy name?"
No. Co-location means a therapist works in the same building as a primary care clinic but operates independently. CoCM requires systematic care coordination: shared registries, standardized outcome tracking, and regular psychiatric consultation. The model is protocol-driven, not ad hoc.
"Do patients have to consent to seeing a psychiatrist?"
Patients consent to CoCM enrollment, which includes psychiatric consultation. They understand that a psychiatric consultant will review their case with the care team, but they don't meet the consultant directly in most programs. This often reduces stigma because it normalizes psychiatric expertise as part of routine medical care.
"What if a patient needs more intensive therapy than brief interventions?"
CoCM is designed for mild-to-moderate depression and anxiety: the conditions that show up most often in primary care. Patients with severe mental illness, active suicidal ideation, or complex trauma get referred to specialty mental health clinics. The care manager helps coordinate those transitions.
"Can CoCM work in private practice or only in large health systems?"
Independent practices can implement CoCM, but it's easier at scale. You need at least 2–3 PCPs generating enough patient volume to justify a full-time care manager. Many small practices join accountable care organizations (ACOs) or partner with larger networks to share a care manager and psychiatric consultant.
"What credentials should I require for a Behavioral Health Care Manager?"
Most programs require an LCSW, LPC, or LMFT with independent clinical licensure. Some use RNs with psychiatric training, especially in integrated medical settings. Avoid requiring PhD-level clinicians; the role is care coordination, not long-term psychotherapy.
Finding CoCM Talent: What to Look For
When you're hiring for a CoCM team, you're not only filling traditional behavioral health roles.
You are recruiting for a specific care model for behavioral health services with distinct competencies.
For Behavioral Health Care Managers:
- Experience with brief interventions (behavioral activation, motivational interviewing, problem-solving therapy)
- Comfort with outcome measurement and data tracking
- Willingness to work in a medical clinic environment
- Strong communication skills for presenting cases to psychiatric consultants
- Ability to manage a high-volume caseload with structured workflows
For Psychiatric Consultants:
- Board certification in psychiatry or PMHNP certification
- Experience reviewing cases remotely (not direct patient care)
- Comfort with curbside consultation and real-time decision support
- Knowledge of primary care prescribing patterns
- Licensure in states where your clinics operate (or eligibility for PSYPACT/Counseling Compact)
Where to Post These Jobs
Use BehavioralHealth.careers to reach clinicians who understand integrated care models. Tag your listings with "Collaborative Care Model," "Integrated Behavioral Health," or "Care Manager" to attract candidates with the right experience.
Include salary ranges: care managers typically earn $60,000–$85,000 depending on region and licensure level, while psychiatric consultants earn $200,000–$280,000 for full-time consulting roles.
The CoCM workforce is growing, but it's still specialized. If you're hiring in 2026, you're competing for a finite pool of clinicians who understand registry-based care and measurement-driven treatment to improve clinical outcomes as well as patient satisfaction.
Make your job posts explicit about the model, the caseload structure, and the support systems in place. Clinicians burned out on traditional therapy models are actively looking for CoCM roles: you just need to reach them where they're searching.